10th July 2020
Hi Debbie,
Trying to condense the points from the June email with attachments I sent you.
Going forward what we would like now is – for you to approach key people involved in the discussions who can push this forward quickly and formulate a plan of how to get Herceptin approved in 3rd+ lines aswell as review lapatinib and additional issues highlighted below.
We feel there are 2 issues, one specifically with Herceptin (Traztuzamab) aswell as general access to drugs and then it raises further policy and procedures for Herceptin, lapatinib and other drugs which will be eventually approved.
Herceptin unmet need
Lack of a NICE guidance review in the eighteen years since Herceptin’s approval. It is possible to accelerate review, approval and access?
First we need an urgent Rapid Review by NICE for this Unmet need for Herceptin 3rd and subsequent lines
The manufacturer, of Herceptin, Roche, has no incentive to request a Rapid Review for a now off patent drug.
There is a lack of access to data to request a review by the NICE (overwhelming data does exist from several source points from many clinical trials for HER2+ patients)
Herceptin is widely used as the SOC – Standard of Care – treatment “arm” in clinical trials. So patients who have had many lines of treatment will be offered Herceptin in clinical trials. When you sign the contract for a clinical trial, it clearly states proven safety and efficacy.
Alternative drugs such as biosimilars are cheaper, but the price is still inflated. However, the price still falls within the NICE QALY (Quality Adjusted Life Year) model and Roche wont provide data as they see these manufacturers as competition and wont give them historical data
Colin’s petition has over 20k signatures.
Cally Palmer & John Stewart have ignored emails since April and still not replied
James Grundy MP has advised Colin to take the complaint about lack of response by Cally and John to the Ombudsman
We believe Prof Peter Clark who has been part of NICE technology appraisal committee 2009-2013 could be KEY with raising this issue at a higher level.
Melanie Sturtevant from BCN Policy needs contacting re NHSE commissioning to see where she is up to with her application – we do not want delays or rejection
Evidence does exist for the use of Herceptin in later lines (see Prof Carlo Palmeri and Dr Tim Robinson report) therefore we need this data (in the USA around 2 million patients have had this drug 3rd line 4th line etc therefore how to Roche say there is no data? There is worldwide data in abundance.
Roche has denied “compassionate access” citing there are too many women in the same position (approx 3000 women who need this drug with metastatic disease) and it is an unmet need
Herceptin is SOC – standard of care in many other countries and in different drug lines. Additionally Roche still have the patent on the subcutaneous version of Herceptin.
Clinical trials – all have Herceptin included in whatever drug the trial specifies and we understand Herceptin gives 70% benefit to patients with HER2+ SBC – chemotherapy alone will not deliver the same results.
Roche advised that they are not the sponsor for many of these studies and does not have the resulting data – how can this be true?
NICE has not reviewed the data on Herceptin since 2002 and many things have changed with new advances but the drug is still very relevant in HER2+ SBC patients
There are now double and triple drug combinations of this drug with others so a QALY needs to keep up with the drug cost as this could out price effective drug combinations?
Policy and access issues
There are disparities between access for private and NHS patients. (And across countries, England, Wales, Scotland, Ireland) This is discrimination.
There are major delays in the UK within the approval process for access to new drugs.
New drug Enhertu is in the pipeline – will it be available only 3rd line? This drug needs to be available any line of treatment.
New drug Tucatinib it important for HER2+ patient who have brain mets as this is a huge UNMET NEED
This is all down to market share – drugs are combined with Herceptin and sold as a package and roche will not loose out due to these new drugs becoming available ie above mentioned Enhertu and Tucatinib
Lapatinib needs to be made available due to the fact this drug is used in ALL SOC clinical trials. It was taken off the CDF and it needs to be part of SOC. Denying this drug in SOC could mean that it is a human rights issue. Jennifer was denied this drug after she had it in a clinical trial and was denied to stay on the drug even though she had not progressed. This could have given her additional months on this line of therapy. This is wrong.
Data is in the private healthcare setting for Herceptin and lapabinib. We need this data releasing.
We are missing out on new drugs due to the system being not fit for purpose to appraise new medicines correctly. (see ICR Report 2 years ago)
Are the NHS here to improve survival for SBC patients? There are many similar issues with other cancers like bowel, lung and prostate.
Patients are progressed and pushed through lines of treatment to an earlier death instead of looking at being on a drug and having surgery or radiotherapy or other treatment in addition to any line of drug. We need lines of treatment to be quashed. Oncologists are the EXPERTS but give them “guidance”.
Pharmacy Depts in hospitals are blocking oncology advice and advising to push patients onto next lines of treatment instead of leaving this decision to an oncologist
Additionally if a patient had NHS treatment and also has some private drug then these drugs should all be delivered in the NHS setting as patients then end up with 2 appointments in 2 separate hosptials for something that usually is delivered in one appointment. Coordination needs to happen better even if the NHS bill PHC for the cost of the time they are in treatment aswell as the cost of the drug.
IFR process had a lot of ambiguity related to what is deemed as “exceptional” I have shared a tweet with Lesley Smith from NHS England who is the Living with and beyond cancer Manager and waiting for a response to an email as a FOI has been requested and apparently only 3% of IFRs are supported so this system is NOT working.
Debbie, as you can see there are lots of issues here but all these problems are connected to the same and wider problem of drug access for ALL cancer patients and supporting patients who have been given a diagnosis of having an incurable illness.
All I can say is that from my own experience and many others in my SBC network, if we get these changes for HER2+ many patients will be living longer with HER2+ disease. We are told with SBC that we have a median life expectancy of 2-3 years. That’s a death sentence. BUT we know all these thing applied correctly our lives CAN be extended. It feels in the UK we are NOT keeping up with new drugs and technologies that are there to extend lives and that should be the primary focus. Secondary Breast Cancer is the biggest killer of women under 50. We need change for all SBC patients and for ALL cancer patients.
COVID has shown that things can be changed rapidly to save lives. Lets now apply that URGENCY to cancer.
Best wishes
Jo Taylor
Founder METUPUK
__________________________________________________________
2nd June 2020
Dear Debbie,
RE: ACCESS TO BREAST CANCER DRUGS INCLUDING TRAZTUZUMAB (HERCEPTIN): SERIOUS PROBLEMS IN THE UK .
FOLLOW-UP TO OUR MEETING, FEBRUARY 2020, LONDON
It was a pleasure to meet you back in February at the House of Commons, and I do hope you and your family are safe and well during these difficult times of COVID-19.
It is an extremely difficult time for those who I represent: Secondary Breast Cancer (SBC) patients living with incurable cancer. Every day we hear that cancer treatments and surgeries are being delayed, and clinical trials set aside because of Covid-19. Cancer patients understand Covid-19 risks, but the extra stress levels this is generating are serious.
However, even before Covid-19, our research shows there are very serious problems with access to breast cancer drugs across the UK – in particular Traztuzumab (Herceptin). Herceptin was developed, licensed and approved for secondary breast cancer in 2002 (refer to NICE – National Institute for Health and Care – guidance TA34 15TH March 2002), so we do not understand why continued access is such an issue.
We are also very concerned at the lack of a NICE guidance review in the eighteen years since Herceptin’s approval for its setting. Herceptin is a $68 billion per annum market for pharmaceutical company, Roche. It is extremely illuminating to note that because of COVID-19, clinical trials and NICE guidelines have been speeded up massively, and where necessary changed, to provide a new drug more quickly to the public. So, it is possible to accelerate review, approval and access.
We really need your help and support to raise awareness and see how we can take action on this lack of access and help increase ‘SBC patients’ life expectancy. Our position is that first we need an urgent Rapid Review by NICE for this Unmet need for Herceptin 3rd and subsequent lines of treatment for SBC patients. Then we need much better and quicker access to alternative and new drugs that are already approved and Standard of Care (SOC) across the world.
There are six key reasons why this is not happening. Please see Annex I attached for more details:
1) The manufacturer, of Herceptin, Roche, has no incentive to request a Rapid Review for a now off patent drug.
2) There is a lack of access to data to request a review by the NICE (overwhelming data does exist from several source points from many clinical trials for HER2+ patients)
3) Herceptin is widely used as the SOC – Standard of Care – treatment “arm” in clinical trials. So patients who have had many lines of treatment will be offered Herceptin in clinical trials. When you sign the contract for a clinical trial, it clearly states proven safety and efficacy.
4) Alternative drugs such as biosimilars are cheaper, but the price is still inflated. However, the price still falls within the NICE QALY (Quality Adjusted Life Year) model.
5) There are disparities between access for private and NHS patients. (And across countries) This is discrimination.
6) There are major delays in the UK within the approval process for access to new drugs.
Steps taken so far:
• I wrote to the Greater Manchester Breast Pathway Board in June 2019 regarding access to Herceptin 3rd line and subsequent line (email attached) but I did not get an official response. I went to the meetings and one of last meetings an oncologist had been assigned to look into this but have heard nothing further.
• Colin Dyke whose wife Jennifer Hall has had SBC for six years, and is under the same oncologist as myself at The Christie, has created a petition: https://www.change.org/p/nhs-england-access-to-a-life-extending-nhs-standard-of-care-drug-herceptin
• However, please see in the attached Annex II, the email from Colin to Ms. Cally Palmer, NHS National Cancer Director regarding his wife’s issues with 3rd line+ access to Herceptin. The response of 4th April from Ms. Palmer’s executive assistant was extremely disappointing as it was a holding email to say Ms. Palmer would respond after “things get easier with the pandemic.” As you can see it has now been six weeks since any correspondence.
Ms. Palmer and Mr John Stewart (National Director of Specialised Commissioning) both responded to advise they would reply and never provided any further response.
• To move this issue forward, it needs to be raised at a higher level – we believe Professor Peter Clark who has been part of the NICE technology appraisal committee 2009 – 2013 is someone who can help to do this.
• Breast Cancer Now is aware of this and Ms. Melanie Sturtevant (copied in this email) is the contact in the policy department. Colin Dyke has contacted her through Breast Cancer Now and Melanie has also raised within NHSE Commissioning through her contacts. We have had a response from Melanie who advises that it may take a full year to get this reviewed and even then, there is a possibility that this will be rejected. Melanie has confirmed she is reviewing all other information now.
• Leigh MP, Joanne Platt, was also working on a case before she lost her seat. The new MP, James Grundy, wrote to Colin Dyke on 24th April, 2020, and has advised that he is looking into the issues Colin has raised.
We would welcome your help, advice and guidance on how to influence more directly.
I understand you are extremely busy, but I look forward to hearing from you as soon possible. I would welcome a further discussion via FaceTime or Zoom very soon. Please can you follow up this matter with Jo Churchill as per our discussion back in February. As you can see, there is no time to waste to give secondary breast cancer patients a chance of living longer.
With my best regards,
Mrs. Joanne Taylor
Founder, abcd and METUPUK
Attachments:
(i) This letter in word format
(ii) Annex I: Background Information: Better Access to Drugs to increase people’s life expectancy. Evidence: Why are there access issues?
(iii) Annex II: Letter from Colin Dyke to Dame Cally Palmer, Director for NHS England & NHS Improvement
(iv) Annex III: Clinical Oncology. Editorial: Trastuzumab Beyond Progression in Advanced Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer: UK Practice now and in the Future. T. Robinson, C. Palmieri, J.P. Braybrooke.
ANNEX I
BACKGROUND INFORMATION: BETTER ACCESS TO DRUGS TO INCREASE PEOPLE’S LIFE EXPECTANCY
Evidence: Why are there access issues?
MANUFACTURER: ROCHE
• The manufacturer of Herceptin, Roche, states that it does not have enough data on Herceptin to take this issue to the NICE for a “Rapid Review” to show how many patients are accessing it 3rd, 4th line etc. and prove that there is an ‘unmet need’.
• In a letter to us, Roche said:
‘We have liaised with our UK Regulatory colleagues to seek clarity on how current studies using trastuzumab in combination with chemotherapy in 3+ lines of mBC may potentially impact the Herceptin licence and wider breast cancer guidelines. With regards to updating the Herceptin licence, we acknowledge the studies you have previously referenced, which provide evidence on the use of trastuzumab with chemotherapy for HER2+ve mBC. However, Roche is not the sponsor of many of these studies and therefore does not have access to the resulting clinical data. Full access and ownership of this clinical data is essential to gather the evidence required to apply for a licence extension with the European Medicines Agency (EMA)”.
• However, the evidence does exist for the continued use of Trastuzumab in later lines of Treatment for heavily pre-treated Her2+ MBC patients. In their view it will open another market for the cheaper Bio similar products also there are now newer relevant and deemed as effective products coming to market for Her2+ later lines of Treatment. Roche of course still have a patent on the current sub cut version of Herceptin, which is very expensive.
• We think Roche has no monetary incentive to push a Rapid Review because Herceptin has now come off patent. The evidence does exist for the continued use of Trastuzumab in later lines of Treatment for heavily pre-treated Her2+ MBC patients.
• Roche has also refused to give “compassionate access” to the drug for patients who really need it citing there are too many women in the same position, which in our opinion, it itself shows actually that there is an ‘Unmet need.”
LACK OF DATA and LACK OF ACCESS TO DATA:
• There is no data and statistics available for this line of therapy currently for us to provide to NICE.
• However, in the USA in the past 10 years, over 2 million patients have had access to this drug many 3rd, 4th line treatment so it is hard to accept Roche saying, “we don’t have the data”.
• The drug is already approved as SOC in many different drug lines and in many other countries.
• Also, in the USA & the UK, ALL clinical trials going forward for HER2+ patients have Herceptin included with whatever drug they combine it with. My oncologist states that addition of Herceptin gives additional 70% benefit to patients.
• The problem is that NICE has not reviewed the data on Herceptin since 2002. There needs to be an urgent review of this due to biosimilars and the need for 3rd line and after.
• NICE needs to keep up to date reviews with treatments and therapies. It only seems to be when a new drug is available that there is a review.
• Prof. Carlo Palmieri and Dr Tim Robinson have created a survey so that clinicians can ANONYMOUSLY answer whether they are prescribing Herceptin 3rd and 4th line for patients so that they can collect the data. The results have now been accepted and have now been published here: https://www.clinicaloncologyonline.net/article/S0936-6555(20)30186-2/pdf (attached copy in Annex III)
• Some drugs are now targeted for dual and triple combinations so how are they to be assessed especially when this then takes drug costs over the QALY (Quality Adjusted Life Year) or disease burden.
BIOSIMILARS:
• Biosimilars to Herceptin are now widely used in UK hospitals. Biosimilars are 25% cheaper. This should mean that the cost has reduced considerably. However, we find that this is not the case and the price is kept inflated. We believe there are two issues:
(i) The manufacturers of biosimilars do not have historical data, which for intellectual property reasons remains with the original manufacturer. Therefore, there is a perpetual circle of no data, no information, no evidence, can’t review it if no data.
(ii) Some small hospitals “fudge it” and gain access for patients “under the radar.” However, large and more publicly prominent hospitals like The Christie, Manchester, and The Royal Marsden, London cannot do this. They have to go by the rules and cannot get patients 3rd and 4th line Herceptin.
NEW DATA, NEW DRUGS, NEW CLINICAL TRIALS:
• There are new data available from the following trials: Destiny Breast and Her2climb, Tulip trial etc. which were reported at San Antonio Breast Cancer Symposium 2019
o #HER2CLIMB tucatinib :
o #SOPHIA margetuximab
o #DESTINY-breast01 (DS-8201)
o #APHINITY adjuvent pertuzumab
o #ATEMPT T-DM1 vs. TH (trastuzumab emtansine (T-DM1) and paclitaxel/trastuzumab (TH)
• In addition, there are new drugs just introduced through the USA FDA called Enhertu and Tucatinib. Patients now have access to these leading-edge new drugs, but the UK does not. These will have to go through the NICE appraisal process for a review to check cost vs. clinical benefit. These drugs will not be available in the short to medium term for SBC patients. it could take years for approval.
• These drugs are licenced and patented with Herceptin. Therefore, Roche will not lose market share and profits due to Herceptin coming off licencing. These new drugs will increase their profits.
• This information below is from a trial held in the UK. The Tulip Trial vs SOC – Standard Of Care. See the physician’s choice in the clinical trials, but the issue is we don’t have these offered on 3rd plus lines of treatment. Again, lapatinib not available via NHS and we cannot have Herceptin with chemotherapy, yet in the NHSE contract that the patient signs to enter the Trial it says that these drugs have proven safety and efficacy. They should also be SOC within NHSE. That is a fact.
TWO-TIER SYSTEM IN THE UK: PRIVATE VS. NHS PATIENTS
In the UK, there is a two-tier system. There are private patients who are paying for access to these drugs in certain ways or combinations that their oncologist deems necessary. Standard NHSE patients cannot access drugs in this way.
NHSE patients are being denied life-extending drugs like Herceptin that are already being used widely in the private sector and worldwide as SOC. In NHSE we still operate under NICE and commissioning guidelines generally only allowing two lines of treatment. This is discrimination. There is a lack of approved later line treatments within NHSE for SBC patients that is impacting how long patients will live for and no doubt, shortening life expectancy in many cases.
DELAYS IN UK FOR ACCESS TO NEW DRUGS
There are amazing drugs and new therapies that are approved in the USA by the FDA and pushed through quickly to support patients to live longer. However, it is taking YEARS sometimes for them to be made available for UK patients. We are missing out on advances in medicine to improve and increase survival in patients with secondary cancer. There will be similar issues with lots of cancers like bowel cancer, lung cancer etc.
FDA drugs for HER2+ patients
Patients are progressed and pushed through lines of treatment it seems to an earlier death.
The Institute for Cancer Research (ICR) reviewed this issue in 2019 and reported this recently here: https://www.icr.ac.uk/news-archive/most-innovative-cancer-drugs-facing-delays-in-reaching-patients
Patient to patient review
https://d1ijoxngr27nfi.cloudfront.net/docs/default-source/default-document-library/from-patent-to-patient.pdf?sfvrsn=8fa95f69_4
This detail is specified in the report for breast cancer: –
• “A total of 15 drugs were licensed for breast cancer from 2000 to 2016 – six from 2000 to 2008 and nine from 2009 to 2016.
• A range of targeted drugs have been licensed including monoclonal antibodies such as trastuzumab (also known as Herceptin), pertuzumab and bevacizumab, and the small-molecule inhibitors palbociclib and lapatinib. Among the other authorisations, a new cytotoxic chemotherapy called eribulin mesylate, which is based on a substance derived from a marine sponge, was approved for women with advanced breast cancer.”
NOTE: Lapatinib has now been taken off access via the Cancer Drug Fund (CDF) . Why has this happened when this is a drug that can help with brain mets and from our understanding there are not many from which to choose. “lapatinib, a small-molecule HER2 inhibitor that was licensed in 2008 for the treatment of patients with advanced metastatic breast cancer in combination with trastuzumab (Herceptin) but has still not been appraised by NICE for this indication” Lapatinib needs an appraisal and needs to be part of the standard of care.
Lapatinib is used as a comparable clinical trial “Standard of Care” vs. a tested new drug, so how is it possible that this can be called SOC (Standard of Care) when in the UK we don’t even have access to it? Could this be a human rights issue? (see the details above regarding the Tulip trial and my comments).
Jennifer Dyke had an excellent response on Lapatinib within the clinical trial (SOC) for nine months. She was told that even though there was minor growth, if it were SOC within NHSE, she would have been kept on it. (Very strict Trial protocol).
ICR have provided a drug manifesto:
https://www.icr.ac.uk/about-us/policy-and-engagement/cancer-drug-manifesto
Annex II
Letter below from Colin Dyke to Dame Cally Palmer
Director for NHS England & NHS Improvement
Chief Executive, The Royal Marsden NHS Foundation Trust & National Cancer
Hi Rebecca and Diane,
We hope you and your family/friends are safe, in these incredibly difficult times. Our gratitude is to those key frontline workers (NHS) who are supporting our country day in and day out. Jennifer and I are very grateful and very thankful to The Christie, for the great service they continue to provide on Cancer care.
Whilst we fully understand the current situation, which actually feels like many of the emotions mentally, physically, psychologically, clinically and financially we go through most days, we cannot stop our campaign fighting for change for the better.
We wanted to conclude with a final summary for John and Cally, summarising all of the relevant / key information.
It’s very difficult for us all at the moment but the lack of response from the individuals who are empowered to really make a difference, makes it even harder.
It is also very distressing for us that we continue to go into debt to fund a life extending drug that should be available to Jennifer via the NHS.
John could pick up the phone today and tell Chris Harrison of The Christie (Who he knows) to support this important drug for Jennifer for at least the next few months and until her next scan. She is currently doing well on the combination including Trastazumab.
We live in hope.
So in summary:
Dear John and Cally, We now have over 20,000 supporters for our campaign. http://chng.it/rFk2DkXc
If we start with the premise, as stated below, from a our respected expert NHS Oncologist of over thirty years and with seventeen years+ within The Christie NHS world renown foundation trust;
Now the real Issue;
A complete lack of later line Treatments within NHSE, for this group of patients with Her2+ MBC, who have been previously, heavily pre treated.
There is an ‘Unmet’ need here in the UK relating to heavily pre treated Her2+ MBC patients, of which there are 1,000s. The ‘Unmet’ need is for the approved use, in later lines of Treatment, using the Monoclonol agent Trastazumab, but also, for a quicker approval process relating to the recent FDA Her2+ drug approvals (Enhertu, Neratinib and Tucatinib is currently being fast tracked). Lapatinib is also a proven later line Treatment option, (See below). As stated, NHSE has refused to accept the recommendation of their trusted Oncologist Dr Greg Wilson. He is not being permitted to prescribe the life extending drug Trastazumab in an off label later line setting, to Jennifer, within NHSE.
There are very limited Treatment options available for Jennifer yet she responds very well to regimens and remains relatively fit with a good QoL.
NICE / Commissioning guidelines prevent later lines of Treatment, using Trastuzumab though we know it is actually being widely used within NHSE, privately and worldwide in later line settings and within the majority of Her2+ related Trials as SOC and in heavily pre treated patients.
Extract from the recent Tulip Trial T&Cs that Jennifer was thankfully involved within :-
Lapatinib also worked extremely well for Jennifer and over an eight month period within the Trial. It is not an approved SOC option within NHSE.
Interesting recent study below on Lapatinib. The Trial team stated that if Lapatinib had been approved as SOC within the NHS, Jennifer would have continued on the combination within the NHS on leaving the Trial.
How can drugs be used as SOC and as the standard drug physicians would supposedly use everyday, within the Trial and in comparison to the Trial drug , if in reality, the comparator is not a SOC drug being used within the NHS in the required setting that the novel Trial drug is being assessed for future use for. It does not make sense.
https://www.practiceupdate.com/content/lapatinib-and-treatment-after-lapatinib-in-patients-with-previously-treated-her2-positive-metastatic-breast-cancer/97127 Jennifer has been under Dr Wilson for six years and thanks to his Treatment plans and excellent care, Jennifer is alive today with a good QoL. We do know that NHSE prescribe other Cancer related drugs, in the ‘Off label’ setting’. I.E
We also know that Dr Wilson is confident that Jennifer’s proposed new personalised Treatment plan, has a high probability of delivering remission. This given his real life working experience using Trastuzumab over many years in combination with chemotherapy within his private clinics, including The Christie private clinic.
As we have stated over the past year, in much of our correspondence to our MP, NHSE, NICE, Roche, The Christie and others, the evidence clearly shows that Trastazumab should not be rationed to just two or three or four lines of treatment within NHSE. Her2+ MBC patients need Her2+ directed therapy for the chemotherapy to work and provide maximum efficacy. There are many options at your disposal to address this ‘Unmet’ need, in a sensible logical and ethical manner. A change to the outdated 2002 NICE guideline will really help the 1000s of women in the UK, who need a Her2+ monoclonal therapy in late Stage MBC. Chemotherapy alone will not deliver the same results. We have offered several solutions and compromises to gain support for the 1000s that need this important drug, yet seemingly, this has fallen on deaf ears. On going Treatment options for this group are extremely limited within NHSE. This needs to change quickly. There are now four bio-similar Trastuzumab drugs within the market and the QYAL is now well below the £20K NICE guidelines. We are sure Blake Dark has excellent commercial agreements in place for all these Trastuzumab options. The product cost alone is probably a lot less than we are now having to pay for Kanjinti, including the service to administer the drug (See below). Also, from our perspective the Ms Rogers 2006 Herceptin case albeit for EBC should have provided enough clarity for any similar type of scenario not being repeated. I.E the denying of critical access, to a life extending drug. Especially given the current evidence within recent Trials and the FDA approval of new Her2+ DT drugs, for heavily pre treated patients. (Enhertu, Neratinib, Tucatinib, Lapatinib, NALA Trial, SYD985 Trial, Destiny 1/2/3/4 Trials).
There is worldwide supporting data in abundance.
As stated above, Trastazumab is also used as SOC in all these Trials and then either within the (Conjugate) or in combination with the new approved drugs. How much proof does one need. These new drugs need to be fast tracked through the EAMs scheme and or into the CDF (ASAP).
Relevant drug articles:-
CDF:-
Is Blake Dark also working hard with manufacturers to get patient access to the new life extending drugs quicker, via the NICE scheme below;
https://www.nice.org.uk/about/what-we-do/patient-access-schemes-liaison-unit Every indicator we look at and review, in a very logical, balanced and sensible manner, points to the ‘Clinical need’ for Trastazumab being a SOC option within the NHS for heavily pre treated MBC patients who are Her2+ but also, a policy amendment to include a sensible number of lines of protocol or no limitation but based on the Oncologist clinical decisions.
(E.G The NICE Eribulin guideline TA423 states, administer until both the clinical physician and patient agree that it is no longer working. Oncologists across the UK who should be your ‘Go too’ advisors, are in full favour of more flexibility with later lines of Treatment using Trastuzumab. In fact, some Trusts already continue to provide Treatment under the radar. It’s not our intention that this should stop, more a policy to ensure fairness for all and no more discrimination. NICE have not reviewed the below guideline in its setting for eighteen years and only extended the license in 2009, versus a full review of the guideline.
The current market is now worth over $7Bn worldwide for this drug.
Trastuzumab is SOC in many countries worldwide and for heavily pre treated Her2+ MBC patients, there are no restrictions on lines of Treatment generally.
We have been in dialogue with Roche over many months providing them relevant information. Roche acknowledge the latest Trials, new drug developments and the current evidence. What they tell us is;
Letter from Roche, key paragraph extract as follows;
We have liaised with our UK Regulatory colleagues to seek clarity on how current studies using trastuzumab in combination with chemotherapy in 3+ lines of mBC may potentially impact the Herceptin licence and wider breast cancer guidelines. With regards to updating the Herceptin licence, we acknowledge the studies you have previously referenced, which provide evidence on the use of trastuzumab with chemotherapy for HER2+ve mBC. However, Roche is not the sponsor of many of these studies and therefore does not have access to the resulting clinical data. Full access and ownership of this clinical data is essential to gather the evidence required to apply for a licence extension with the European Medicines Agency (EMA).
The evidence does exist for the continued use of Trastuzumab in later lines of Treatment for heavily pre treated Her2+ MBC patients.
We feel that the big issue is. Roche do not wish to invest time and money to obtain a new guideline within the license / M.A for a product where the patent has expired. In their view it will open up another market for the cheaper Bio similar products also there are now newer relevant and deemed as effective products coming to market for Her2+ later lines of Treatment. Roche of course still have a patent on the current sub cut version of Herceptin, which is very expensive.
How do we therefore address the ‘Unmet’ need for the 1,000s who need Trastazumab and or the newer treatments recently FDA approved.
As stated below, we are now paying privately for Trastazumab , without it Jennifers NHS trusted Oncologist has stated Chemotherapy alone only has a low probability of achieving remission but administered with Trastuzumab a very high probability.
We survive mainly on universal credit and carers allowance, ultimately, if we have to continue to pay for Treatment then we are accumulating more debt.
Our next point therefore is. We do not want to really use The Christie private clinic, based in The Christie NHS trust hospital. We don’t want to pay this amount of money for a thirty minute infusion. HCA turnover £430M and make £32M profit. They buy their drugs in from Baxter’s this probably keeping the American connection in play. We believe that we should still have the choice to have our full treatment plan managed through The Christie NHS and if required pay for the ‘Top up’ drug Trastazumab and the thirty minute infusion when also receiving the NHS SOC treatment. We are sure that this would be far more cost effective for us and would also help the NHS financially. It also makes sense for one visit to hospital, especially given the Corona virus situation. Our experience within the private clinic was no better than that received within The Christie NHS trust, other than, you are offered a club sandwich. The facility is not as good as the NHS Christie Oak road Treatment centre which is new and leading edge, a fantastic facility with exceptional staff. We would rather pay the NHS directly for ‘Top up’ Trastazumab utilising their huge buying power, versus paying the HCA Christie private clinic £900, (Product cost / inc £350 for the privilege of covering the use of the chair/overheads and profit).
We 100% want to use the NHS fully, for Jennifer’s Treatment plan, that our trusted NHS Oncologist recommends. This given six years of excellent service, the right drug combinations, all coupled with our total faith in our amazing NHS. We note the below policy established in 2009 and wonder whether this is still relevant. Perhaps given eleven years has now past, it needs reviewing ,if this still is the principle / M.O.
https://www.nhs.uk/common-health-questions/nhs-services-and-treatments/if-i-pay-for-private-treatment-how-will-my-nhs-care-be-affected/
We hope that our campaign helps to change what is clearly necessary and very quickly. This to meet the ‘Unmet’ needs of the Her2+ heavily pre treated MBC patient community who are dying prematurely in the UK, due to limited later lines of effective Treatments, using Trastuzumab.
It is important that this large group in the UK have access to the same fair Treatment and care options,that are deemed SOC worldwide and that are also fully available within the private sector or if you personally pay.
It is also important that we achieve ‘Best value for money’ for the UK tax payer, this is a given.
We believe that the Bio similar Trastuzumab products now approved and being used in later lines of Treatment for heavily pre-treated Her2+ MBC patients, deliver on this and of course on the clinical efficacy demanded.
Regarding the IFR process which John recommended we pursue with our Trusted Oncologist. Given the below article, it is clear there is a lot of ambiguity relating to what is deemed as ‘Exceptional’. It is no wonder Trusts and Oncologists are persuaded away from applying through this process. Reading clause 111 in particular, demonstrates to us, that a strong case for Jennifer to receive continued Trastuzumab through NHSE, could be presented for consideration.
https://academic.oup.com/medlaw/article/20/3/304/957776
We also wish to include a very strong and committed advocate blog, relating to many frustrations from the BCC, including the well documented issues around Data. These issues were discussed in a face to face meeting recently, held with Matt Hancock this led by Breast Cancer now.
Very important blog:-
https://twitter.com/abcdiagnosis/status/1235569250187657216?s=21
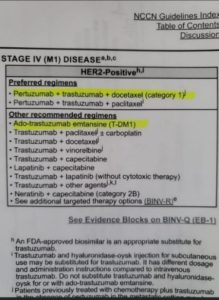
Finally, in a very recent survey held by leading worldwide Oncologists at the largest BCC in Miami and relating to their preference for 3rd line+ Her2+ MBC therapy. The below outlines their preferred regimens. None of these options /combinations are available as SOC within NHSE.
Surely you both agree that this needs addressing given the ‘Unmet’ need for the 1000s of women, in the UK who may die prematurely due to a lack of on going later line treatments which they would benefit from.
Thanks for reading this, we now await your response and any relevant timely key actions.
We are available anytime for relevant feedback or further any questions you may have.
Kind Regards, Colin and Jennifer
HERCEPTIN ANNEX III
https://www.clinicaloncologyonline.net/article/S0936-6555(20)30186-2/fulltext